
Diagnosis and treatment of malignant pleural mesothelioma markers
SUMMARY
The diagnosis of malignant pleural mesothelioma markers presents 3 important challenges: it is necessary to distinguish between benign mesothelial hyperplasia and mesothelioma, between malignant mesothelioma (with subtypes) and metastatic carcinoma, and it is also necessary to demonstrate the invasion of neighboring structures to the pleura. To clarify the first 2 aspects, it is necessary to rely on a panel of monoclonal antibodies with adequate immunohistochemical study – performed by highly expert hands – and for the third, to rely on sufficiently wide and deep biopsies, and thoracoscopy is the technique of choice. Needle biopsy guided with real-time imaging techniques can be of great help when there is marked diffuse nodular thickening and small or absent effusion. Given the difficulties of an early diagnosis, It is uncommon for curative treatment to be achieved through radical surgery (pleuropneumonectomy), which is why in recent years the release of tumor mass through pleurectomy / decortication, with the combination of chemo and radiotherapy with surgical techniques (multimodal therapy), has been gaining popularity. In cases where surgery is not feasible, chemotherapy is considered (combining pemetrexed and platinum compounds in most cases), with pleurodesis or placement of a tunnelled pleural catheter if control of the pleural effusion is required, and reserves radiotherapy for the treatment of pain associated with infiltration of the chest wall or any other neighboring structure. In any case

ABSTRACT
There are three major challenges in the diagnosis of malignant pleural mesothelioma: mesothelioma must be distinguished from benign mesothelial hyperplasia; malignant mesothelioma (and its subtypes) must be distinguished from metastatic carcinoma; and invasion of structures adjacent to the pleura must be demonstrated. The basis for clarifying the first two aspects is determination of a panel of monoclonal antibodies with appropriate immunohistochemical evaluation performed by highly qualified experts. Clarification of the third aspect requires sufficiently abundant, deep biopsy material, for which thoracoscopy is the technique of choice. Video-assisted needle biopsy with real-time imaging can be of great assistance when there is diffuse nodal thickening and scant or absent effusion. Given the difficulties of reaching an early diagnosis, cure is not generally achieved with radical surgery (pleuropneumonectomy), so liberation of the tumor mass with pleurectomy / decortication combined with chemo- or radiation therapy (multimodal treatment) has been gaining followers in recent years. In cases in which surgery is not feasible, chemotherapy (a combination of pemetrexed and platinum-derived compounds, in most cases) with pleurodesis or a tunneled pleural drainage catheter, if control of pleural effusion is required, can be considered. Radiation therapy is reserved for treatment of pain associated with infiltration of the chest wall or any other neighboring structure. In any case, comprehensive support treatment for pain control in specialist units is essential: this acquires particular significance in this type of malignancy. so liberation of the tumor mass with pleurectomy / decortication combined with chemo- or radiation therapy (multimodal treatment) has been gaining followers in recent years. In cases in which surgery is not feasible, chemotherapy (a combination of pemetrexed and platinum-derived compounds, in most cases) with pleurodesis or a tunneled pleural drainage catheter, if control of pleural effusion is required, can be considered. Radiation therapy is reserved for treatment of pain associated with infiltration of the chest wall or any other neighboring structure. In any case, comprehensive support treatment for pain control in specialist units is essential: this acquires particular significance in this type of malignancy. so liberation of the tumor mass with pleurectomy / decortication combined with chemo- or radiation therapy (multimodal treatment) has been gaining followers in recent years. In cases in which surgery is not feasible, chemotherapy (a combination of pemetrexed and platinum-derived compounds, in most cases) with pleurodesis or a tunneled pleural drainage catheter, if control of pleural effusion is required, can be considered. Radiation therapy is reserved for treatment of pain associated with infiltration of the chest wall or any other neighboring structure. In any case, comprehensive support treatment for pain control in specialist units is essential: this acquires particular significance in this type of malignancy.Keywords:Malignant pleural mesotheliomaBiomarkersMalignant pleural effusionThoracoscopy.
Introduction
Mesothelioma is a tumor that derives from the mesodermal surface of the embryonic coelomic cavity, which later will give rise to the pleura, the pericardium, the peritoneum and the tunica vaginalis of the testicle. This mesodermal origin gives it the potential to develop an epithelioid and a sarcomatous component. Since the 1950s, the association of this tumor with asbestos has been known 1, particularly in its “blue asbestos” (or crocidolite) and “white asbestos” (chrysotile) forms, and its relationship with exposure to erionite, which is a natural soil pollutant in various regions of the world, is also well known. in the Cappadocia region (Turkey), where a very high incidence of mesothelioma is observed, probably also associated with a certain genetic susceptibility 2 . In approximately 80% of mesothelioma cases there is a cause-effect relationship with occupational exposure to asbestos, with a wide spectrum of professions involved 3However, possible environmental exposure must also be taken into account, generally due to proximity to mines or factories where the mineral is handled or due to contamination through the clothing of asbestos workers 4 . A dose-response relationship has been demonstrated between cumulative asbestos exposure (high levels of exposure, duration of exposure, or both) and malignant mesothelioma, and there is no threshold below which the risk of contracting the disease is ruled out 5– 7. Mesothelioma can appear in any of the structures of mesodermal origin mentioned above, but the most frequent presentation (in more than 90% of cases) is pleural, although its incidence is relatively low, and ranges between 7 cases per million inhabitants / year in Japan and 40 in Australia, mainly depending on asbestos exposure in past decades 8. In Europe, the incidence is estimated at 20 cases per million / year, with notable variation between countries (also in relation to the history of exposure to asbestos in the past), but in any case a global increase is expected, depending on the long period latency between exposure and manifestation of the disease, which is around 40 years, with a wide margin between extreme values (up to 75 years in the series by Bianchi et al.) 9 . Based on the consumption of asbestos, it has been estimated that the peak of maximum incidence of mesothelioma will be registered around the year 2020 in Europe, with marked differences between countries 10 .
To prepare this article, a search was made in PubMed ( http://www.ncbi.nlm.nih.gov/pubmed ) (updated March 18, 2014) combining the terms malignant+pleural+mesothelioma , and 4,670 articles were found (736 reviews among them). Detailed prospective studies with large series, evidence-based clinical guidelines and some studies on very specific aspects, such as biomarkers or novel techniques with future perspectives, have formed the basis for including the most relevant articles in this review on mesothelioma. malignant pleural.
Diagnosis of malignant pleural mesothelioma
Mesothelioma can initially present with a clinical picture of dyspnea, generally related to the development of pleural effusion, and it is also very frequent that it is accompanied by pleural pain, which is not usually clearly related to respiratory movements. In early stages, weight loss or any other symptoms are rare, although later marked retraction of the hemithorax usually appears, and the pain acquires special intensity and persistence.
Imaging techniques in the diagnosis of mesothelioma
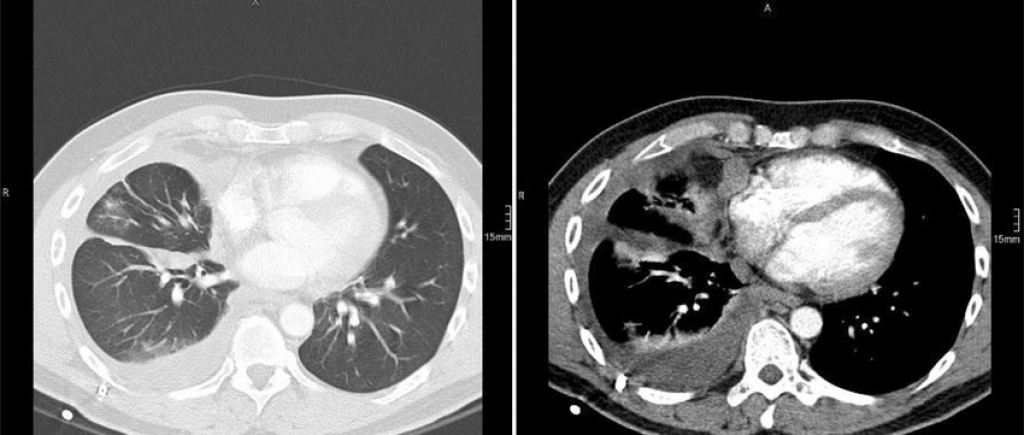
Although the chest X-ray is the first step and can provide us with information on the presence of effusion, diffuse pleural thickening or masses, computed tomography (CT) – preferably with contrast – is essential for the correct evaluation of the patient and the choice of the diagnostic steps to follow: diffuse pleural thickening with nodular prominences suggests mesothelioma, especially in a patient with a history of exposure to asbestos in any of its modalities 11 . However, CT is not very sensitive to assess possible mediastinal lymph node involvement or the existence of contralateral or peritoneal pleural involvement. To investigate these aspects, and the presence of possible distant metastases, positron emission tomography is much more useful (positron emission tomography [PET]), especially when combined with CT (PET-CT) 12 . PET-CT plays an important role in the preoperative staging of malignant pleural mesothelioma, in assessing the response to treatment and to detect the possible occurrence of relapses 13 . However, its sensitivity and specificity are low for detecting N2 disease in mesothelioma 14 , and false positives can be seen in tuberculous pleurisy 15 , empyema 16 or in patients with history of previous pleurodesis 17 .
Nuclear magnetic resonance (NMR) provides a better contrast than CT for defining the invasion of the chest wall mesothelioma, but is not able to reliably detect the presence of metastatic disease 18 .
Pleural fluid study
Thoracentesis can provide some suggestive – but rarely diagnostic – data of mesothelioma: high levels of hyaluronic acid (>100,000ng / ml) are highly suggestive of malignant pleural mesothelioma 19 , and is also attributed a strong prognostic value, so that a high hyaluronic acid is associated with increased survival 20 .
Adenosine deaminase (ADA) levels may be elevated in patients with mesothelioma 21 , but before labeling them as false positives of the ADA, it must be taken into account that malignant mesothelioma and tuberculous pleurisy can sometimes coexist, and therefore it is recommended to do a culture for M. tuberculosis in these cases 22 .
Pleural fluid cytology can reveal the presence of mesothelioma, but it frequently raises problems between benign and malignant mesothelial hyperplasia 23 , and is also unable to demonstrate the invasiveness of the tumor (which is currently considered an essential feature for definitive diagnosis) 24 . However, in rare cases can be combined cytology and imaging techniques to assess the extrapleural invasion 25 . On the other hand, immunocytochemical / histochemical techniques are always necessary to establish the distinction between mesothelioma and metastatic adenocarcinoma in the pleura 26, and this requires tissue obtained by biopsy, or cell blocks prepared by embedding the cell button in paraffin after centrifugation of a sufficient volume of pleural fluid (>100ml). The combination of all the following assumptions can provide the diagnosis of mesothelioma with sufficient reliability: atypical mesothelial proliferation in pleural fluid+immunohistochemical studies consistent with mesothelioma in cell blocks+diffuse pleural thickening with nodulations+absence of masses in the lung or in any other organ suggesting another primary tumor 27 . However, and especially the legal implications involved in the diagnosis of malignant mesothelioma in most cases, and also when surgery poses, try to always get large tissue samples to establish more securely the tumor 28 .
Histological diagnosis of malignant pleural mesothelioma
Classically types are distinguished epithelioid sarcomatous and biphasic in malignant pleural mesothelioma, but also rare subtypes like desmoplastic mesothelioma (which may be confused with fibrous pleuritis benign), the mesothelioma, small cell and linfohistiocitoide mesothelioma (which could be confused with a lymphoma), and immunohistochemical studies are essential to distinguish between them. However, there is no marker with 100% sensitivity and specificity for mesothelioma, and therefore it is essential to go to different panels of monoclonal antibodies, including at least 2 positive markers for mesothelioma (in the epithelioid subtype they would be preferablecalretinin [particularly useful if it stains the nucleus as well as the cytoplasm]), Wilms tumor antigen 1 (WT-1) or epithelial membrane antigen (EMA) or broad spectrum, low molecular weight cytokeratins, such as CK5 or CK6 and 2 negative markers , such as Ber-EP4 (membrane marker) and thyroid transcription factor 1 (TTF-1, nuclear marker). The carcinoembryonic antigen (CEA) is very useful to distinguish metastatic carcinoma —especially of pulmonary origin— from mesothelioma (in which it is practically always negative), and in case of suspected mesothelioma in a woman it is convenient to also investigate the expression of endoplasmic reticulum(ER), which never appears in mesothelioma and does appear in metastatic breast tumors 28 ( Table 1 ) . When the tumor has a sarcomatous component, it is often necessary to distinguish it from metastatic tumors, such as squamous cell lung cancer or transitional cell carcinoma. Although some of the antibodies used for epithelial mesothelioma are also valid for sarcomatous, one often has to rely on different ones, such as p63 and MOC 31 ( Table 2 ).
Table 1.
Immunohistochemical markers to differentiate epithelioid mesothelioma from other metastatic pleural tumors
| Antibody | Diagnostic value | Epithelioid mesothelioma | Adenocarcinoma |
|---|---|---|---|
| Calretinin | Essential | +++ (nucleus and cytoplasm) | ± (cytoplasm) |
| WT-1 | Useful | ++ (nuclear) | (Lung) |
| EMA | Useful | ++ (membrane) | +++ (cytoplasm) |
| CK5 / CK6 Keratins | Useful | ++ (cytoplasm) | – |
| Monoclonal CEA | Very useful | – | ++ (cytoplasm) |
| Ber-EP4 | Very useful | ± (membrane) | +++ (membrane) |
| TTF-1 | Very useful | – | ++ (nucleus, lung) |
| B72.3 | Very useful | – | +++ (cytoplasm, lung) |
| ER | Very useful | – | ++ (nucleus, breast) |
CEA: carcinoembryonic antigen ; EMA: epithelial membrane antigen ; ER: endoplasmic reticulum marker ; TTF-1: thyroid transcription factor-1 ; WT-1: Wilms tumor antigen 1 . Adapted from Scherpereel et al. 28 .Table 2.
Immunohistochemical markers to differentiate sarcomatous mesothelioma from squamous or transitional cell carcinoma
| Antibody | Diagnostic value | Sarcomatous mesothelioma | Squamous or transitional carcinoma |
|---|---|---|---|
| Calretinin | Useful | +++ (nucleus and cytoplasm) | + (cytoplasm) |
| WT-1 | Useful | ++ (nucleus) | |
| CK5 / CK6 Keratins | Not useful | ++ (cytoplasm) | +++ (cytoplasm) |
| p63 | Very useful | – | +++ (nucleus) |
| Ber-EP4 | Very useful | ± (membrane) | +++ (cytoplasm) |
| MOC 31 | Useful | ± (membrane) | +++ (membrane) |
p63: homologous to p53, but more useful for differential diagnosis; WT-1: Wilms tumor antigen 1 . Adapted from Scherpereel et al. 28 .
Pleural biopsy and thoracoscopy for the diagnosis of mesothelioma
“Blind” needle pleural biopsy (without the use of real-time imaging techniques) provides unsatisfactory results for the diagnosis of mesothelioma, not only due to lack of control as to the exact point from which samples are obtained, but also due to the small size of these. When there is diffuse nodular pleural thickening, the performance of needle biopsy can be considerably improved if performed with the help of CT 29,30 or real-time ultrasound 31 . In one study, a diagnostic yield of 75% was achieved in cases where biopsies were>10mm, while only 8% was obtained when they were under 32 , and this clearly advocates thoracoscopy as a diagnostic technique in malignant pleural mesothelioma. Thoracoscopy (or pleuroscopy ) can be performed under local anesthesia and intravenous analgesia / sedation 33 , and we have diagnosed more than 80 pleural mesotheliomas with this method 34 ( Fig. 1 ). The video-assisted thoracoscopic surgery (VATS) allows better staging of the tumor (especially in the mediastinal area) and even make pleurectomía / decortication, but requires more resources, including general anesthesia and tracheal intubation 35. The performance of pleuroscopy (also called “medical thoracoscopy”) is suboptimal in mesothelioma with a sarcomatous component 36 , and therefore it is preferable to obtain more representative samples by VATS or minithoracotomy 37 .

Figure 1.
Various thoracoscopic aspects of malignant pleural mesothelioma. A. Massive infiltration of the parietal pleura by malignant epithelioid-type mesothelioma. B. Diffuse infiltration of the parietal and visceral pleura by malignant epithelioid-type mesothelioma. C. “Pearl” nodules in massive involvement of the parietal pleura due to epithelioid-type mesothelioma. D. Pleural plaques and masses of sarcomatous mesothelioma in the parietal pleura.(0.21MB).
Early diagnosis in malignant pleural mesothelioma
One of the main challenges we face lies in the fact that, although we have identified the population at risk (individuals exposed in one way or another to asbestos), we currently lack the tools to achieve a sufficiently early diagnosis that allows apply a radical treatment in mesothelioma. This implies the need for biomarkers capable of detecting the disease before effusion or diffuse pleural thickening develops, and for now there are also no imaging techniques with sufficient sensitivity and specificity to achieve this objective.
Biomarkers in the diagnosis of malignant mesothelioma
The biomarker that has received the most attention in recent years is soluble mesothelin , which is closely correlated with tumor size and progression in epithelioid mesothelioma (non-sarcomatous, in which it is usually negative) 38 . However, their values are influenced by renal function, and one of its biggest problems lies in identifying suitable cutting point to distinguish between benign and malignant pleural involvement 39. In any case, it seems clear that mesothelin levels are more useful in pleural fluid than in serum, and this greatly limits its value for early diagnosis in subjects with a history of asbestos exposure but without pleural effusion. Given a low pretest probability of suffering from mesothelioma, low levels of mesothelin can help rule it out, while high levels reinforce the use of more invasive diagnostic techniques in a patient with suspected mesothelioma 40–42 . In any case, it seems that mesothelin is more useful for monitoring treatment than for differential diagnosis in pleural effusions 43 .
Trying to overcome the problems of mesothelin and other markers, it has recently been published that fibulin-3 is able to distinguish between healthy people with a history of exposure to asbestos and patients with mesothelioma, and even between mesothelioma and other malignant or benign processes of the pleura. In a study by Pass et al. fibulin in plasma presented a sensitivity of 96.7% and a specificity of 95.5% for a cut-off point of 52.8ng / ml. When patients with relatively early stage mesothelioma and individuals exposed to asbestos but without evidence of disease were compared, the sensitivity was 100% and the specificity 94.1% for a cut-off point of 46ng / ml fibulin-3 44 . These excellent results still require adequate external validation, and it must also be taken into account that the way in which the samples are extracted and processed can significantly influence the results: in the case of fibulin, its determination in plasma (in which it does not the coagulation process has been activated) is much more reliable than in serum, due to the interactions between thrombin and fibulin, as is also the case with other markers 45 .
In recent years, intensive work has been carried out on gene expression studies in mesothelioma 46 , and considerable emphasis is placed on the expression of certain proteins such as aquaporin- 1, which is related to the selective transport of water through the membrane and with cell proliferation 47 , and the study of micro-RNA ( miRNA ) in mesothelioma also stands out . MiRNAs are short RNAs (17 to 22 nucleotides) —not coding for proteins— that regulate gene expression and play an important role in oncogenesis 48 . They have high tissue specificity to detect the origin of a tumor and also to distinguish mesothelioma from other metastatic tumors of the pleura49 . On the other hand, the detection of miRNA in peripheral blood could make them excellent markers of mesothelioma in the near future 50 .
Treatment of malignant pleural mesothelioma
Pleural mesothelioma tends to have a poor response to chemotherapy and radiation therapy, and surgery is rarely curative, because the tumor is generally diagnosed too late, and therefore careful evaluation of each patient before choosing the best treatment modality is especially important. If radical treatment is being considered, it is critical to assess lung and heart function, the presence of other comorbidity factors, and the physical and psychological state of the patient. The choice between the different therapeutic options is dictated by the clinical situation and the tumor extension studies (TNM) using imaging techniques. However, none of the currently available techniques is accurate enough to ensure the “T” and “N” in malignant pleural mesothelioma.51 . Until a more robust TNM staging is achieved, it is advisable to follow that established by the Union Internationale contre le Cancer (UICC) 52 ( Table 3 ).Table 3.
TNM staging of malignant pleural mesothelioma
| Stadium | Tumor extension |
|---|---|
| T1 | Unilateral involvement of the parietal pleura |
| T1a | Involvement of the parietal pleura, with or without involvement of the mediastinal or diaphragmatic pleura, but without involvement of the visceral pleura |
| T1b | Involvement of the parietal pleura and focal involvement of the visceral |
| T2 | Unilateral involvement of the parietal or visceral pleura, with invasion of the underlying lung or diaphragmatic muscle |
| T3 | Unilateral involvement of any area of the pleura, and with invasion of at least one of the following structures: endothoracic fascia, mediastinal fat, soft tissue of the thoracic wall (focal) or non-transmural invasion of the pericardium |
| T4 | Involvement of any area of the pleura, and with invasion of at least one of the following structures: internal face of the pericardium (with or without effusion), peritoneum, mediastinal structures, contralateral pleura, vertebral column, diffuse invasion of the chest wall (with or without costal destruction) |
| N0 | No node involvement |
| N1 | Ipsilateral bronchopulmonary or hilar lymph node involvement |
| N2 | Ipsilateral involvement of mediastinal nodes, from the a. internal mammary and / or peridiaphragmatic |
| N3 | Contralateral involvement of any of the mediastinal and / or internal mammary and / or supraclavicular lymph node stations |
| M0 | Absence of extrathoracic metastases |
| M1 | Extrathoracic, hematogenous, or non-regional node metastases |
| Stage I | T1aN0 (1A); T1bN0 (1B) |
| Stage II | T2N0 |
| Stage III | Any T3, N1 or N2 |
| Stage IV | Any T4, N3 or M1 |
Adapted from Van Meerbeeck et al. 52 .
Surgical treatment in malignant pleural mesothelioma
The main objective of surgery is to macroscopically resect the entire tumor, assuming that with this a better survival is obtained, and that in patients with macroscopically visible remains of the tumor, survival is lower 53 . However, the accumulated evidence suggests that it is not possible to achieve a complete resection (macro and microscopic) in this tumor, regardless of the surgical technique applied, and for this reason it is accepted that the surgery is oriented to locally control the disease, eliminate pleural effusion, release the lung trapped by the tumor, improve ventilation / perfusion disorders and alleviate pain caused by invasion of the chest wall 54. All these considerations apply especially to type epithelioid mesothelioma, as the sarcomatous or biphasic component has a worse prognosis and is consequently a worse candidate for any surgery 51 .
Extrapleural pneumonectomy
It involves en bloc resection of the lung and parietal pleura, and is usually completed with pericardial and diaphragm resection on that side, in addition to systematic dissection of the mediastinal ganglion chains. Although perioperative mortality is around 5% in centers with extensive experience, it has high morbidity, including cardiac and respiratory complications (which may acquire special relevance due to the unipulmonary situation in which the patient remains after extrapleural pneumonectomy [NEP]), fistula bronchopleural, empyema and bleeding, among others 55,56 . In any case, and due to the usual persistence of macro or microscopic tumor residues, this intervention must be considered within the framework of multimodal therapy, which is supported by the combined use of surgery, chemotherapy and radiotherapy 57 . Hyperthermia – combined with chemotherapy – or local photodynamic therapy 58 has also been used occasionally . In many protocols multimodal therapy chemotherapy given as induction therapy before surgery (neoadjuvant chemotherapy), and after resection radiation is applied on the affected hemithorax 59 . However, the most recent clinical guidelines recommend not to intervene surgically if progress of the disease is observed after neoadjuvant chemotherapy and, in any case, they recommend that PSN be performed only in the context of well-controlled clinical trials and by groups specialized in this technique 27,28.
Pleurectomy / decortication
Although it is associated with a higher risk of local recurrence than PNE, it presents fewer complications than that 60 , and is mainly oriented to free the lung and the chest wall from the constriction caused by the tumor. Patients with diffuse macroscopic tumor is in the parietal pleura, but only focus on the visceral, are the best candidates for this surgery 54 . It can be performed using VATS, which has the advantage of minimizing the morbidity associated with thoracotomy 61 and the possibility of performing pleurodesis in the same act if the resection cannot be completed.
PSN offers a more radical approach, but its advantages over pleurectomy / decortication have been widely questioned in recent years 62,63 and a recent randomized study in the United Kingdom ( Mesothelioma and Radical Surgery [MARS] study) did not demonstrated the superiority of one over the other 64 . On the other hand, the MARS study has been harshly criticized for the significant deviations that occurred from the protocol initially proposed and for the number of patients who were finally included in each of the study branches 65. In any case, and although for some groups with extensive experience in both techniques it is considered inappropriate to leave the macroscopically visible tumor unresected (which leads to a worse prognosis), 54 the idea of resecting the largest possible volume of the tumor is gaining adherents, but preserving the underlying lung, and in any case combining surgery with chemotherapy and radiotherapy, within the framework of trimodal therapy 66 .
Radiation therapy in malignant pleural mesothelioma
Radical radiotherapy applied to an entire hemithorax is seriously limited by the risk of damaging critical organs such as the lung, liver, heart, spinal cord and esophagus, and to alleviate this, application techniques are being optimized 67 , although there is no convincing evidence that it alone prolongs the survival of patients with mesothelioma 68 . On the other hand, palliative radiotherapy plays an important role in controlling pain caused by infiltration of the chest wall 69,70 . Prophylactic radiotherapy had traditionally been recommended to avoid tumor seeding in thoracoscopy or thoracotomy scars 71,72However, this practice is not supported by the available evidence, and is currently discouraged 27,28 .
Chemotherapy, immunotherapy and other personalized therapies
Recent clinical guidelines recommend not delaying the administration of chemotherapy, and it should be taken into consideration before functional deterioration of the patient appears 27,28 . The combination of several agents (including pemetrexed and platinum compounds) generally produces better results than monotherapy 73,74 . The current trend is aimed at investigating new therapeutic targets focused on controlling angiogenesis and apoptotic pathways through specific ligands, including platelet derived growth factor (PDGF, which is overexpressed quite frequently in mesothelioma and is associated with lower survival) and mesothelin ( which is expressed only in the epithelial subtype) among others75.76 . Also within multimodal therapy, immunotherapy can play an important role in the treatment of mesothelioma, because this tumor is capable of evading the immune system through T-regulatory cells (Treg) and M2 macrophages, and new therapeutic strategies that combine the Surgical debulking, chemotherapy, immunotherapy and radiotherapy can achieve better control of the disease 77 . From passive immunotherapy (using specific cytokines or antibodies) to modulation of the immune response by dendritic cells or others, there is a wide spectrum of possibilities to achieve markedly synergistic antitumor effects 78–80 .
Pleurodesis
Control of pleural effusion is a priority in most patients with malignant pleural mesothelioma, and talc pleurodesis may be a good option. However, in our experience tend to occur more failures pleurodesis in this tumor than others, and this could be attributed to the inability to properly re-expand the lung, cloistered by the tumor 81 . Thus, previous studies by our group show that the extension of the tumor in the pleural cavity has a negative influence on pleurodesis 82 . However, other biological factors not well known to date are likely to play a role as well. According to recent in vitro experiments By our group, malignant mesothelial cells are more resistant to the action of talc than other cell lines, and this is evidenced both in modulation / blocking of angiogenesis and in cell proliferation (unpublished data).
When pleurodesis fails, or if it is considered not feasible due to the presence of a lung massively trapped by the tumor, the best option is the placement of a tunnelled pleural catheter , which allows the home evacuation of pleural fluid and induces spontaneous pleurodesis in a considerable proportion of cases 83–86 .
It is important to bear in mind that prior pleurodesis does not prevent surgical resection in the case of mesothelioma, regardless of the technique used (PNE or pleurectomy / decortication) 54 .
Future perspectives
Combining molecular biology and nanotechnology techniques, the concept of theranostics has emerged in recent years , which aims to unite diagnosis and treatment in the same procedure through the use of drugs specifically directed to each neoplasm phenotype. If suitable ligands could be found, they could be applied for the early diagnosis of mesothelioma using PET or single photon emission computed tomography (SPECT) 87–89 . Probes combined with highly sensitive biofluorescent techniques have already been developed and are capable of detecting tumors in animal models 90,91 , and there are also techniques based on labeled antibodies or nanoparticles.for use with nuclear magnetic resonance 92,93 , and all this presents a good horizon for its application in humans in the future. Until this happens, it seems more realistic to dedicate itself to the search for detectable markers in peripheral blood and that have adequate sensitivity and specificity for the diagnosis of malignant mesothelioma. Within this line, the most promising field of research is —together with imaging techniques— the exhaustive search for early mesothelioma markers using proteomic techniques , which simultaneously analyze the profiles of a large number of proteins (more than 1,000) and will make it possible to prepare panels configured to achieve maximum diagnostic sensitivity and specificity 94.95 . As explained above, thedetection of miRNA in peripheral blood is also another emerging field to achieve a sufficiently early diagnosis in mesothelioma.
In many cases, the use of gene therapy in mesothelioma has been considered to compensate for the limited efficacy of immunotherapy when the tumor is locally very advanced. To do this, different strategies are used, such as the use of «suicide genes» (which transfer to the tumor the ability to become sensitive to certain drugs), the administration of oncosuppressive genes or the transfer of immunomodulatory genes to the pleural space 96–99. Although its clinical application has so far obtained rather disappointing results due to problems related to the vectors used and its relative inefficiency in controlling a large tumor mass, it is very likely that the inclusion of gene therapy in the multimodal strategy and its combination with techniques based on Nanotechnology contributes very significantly to improving the prospects for treatment of malignant pleural mesothelioma in the future.
Conflict of interests
The author declares no conflict of interest.
BIBLIOGRAPHY
[1]JC Wagner, CA Sleggs, P. Marchand.Diffuse pleural mesothelioma and asbestos exposure in the North Western Cape Province.Br J Ind Med, 17 (1960), pp. 260-271Medline
[2]I. Roushdy-Hammady, J. Siegel, S. Emri, JR Testa, M. Carbone.Genetic-susceptibility factor and malignant mesothelioma in the Cappadocian region of Turkey.Lancet, 357 (2001), pp. 444-445http://dx.doi.org/10.1016/S0140-6736(00)04013-7 | Medline[3]I. Isidro Montes, K. Abu Shams, E. Alday, JL Carretero Sastre, J. Ferrer Sancho, A. Freixa Blanxart, et al .Regulations on asbestos and its pleuropulmonary diseases.Arch Bronconeumol, 41 (2005), pp. 153-168Medline
[4]J. Tarrés, R. Abós-Herrándiz, C. Albertí, X. Martínez-Artés, M. Rosell-Murphy, I. García-Allas, et al .Asbestos disease in a town near a fiber cement factory.Arch Bronconeumol, 45 (2009), pp. 429-434http://dx.doi.org/10.1016/j.arbres.2009.04.007 | Medline[5]Y. Iwatsubo, JC Pairon, C. Boutin, O. Ménard, N. Massin, D. Caillaud, et al .Pleural mesothelioma: Dose-response relation at low levels of asbestos exposure in a French population-based case-control study.Am J Epidemiol, 148 (1998), pp. 133-142Medline[6]G. Hillerdal.Mesothelioma: Cases associated with non-occupational and low dose exposures.Occup Environ Med, 56 (1999), pp. 505-513Medline[7]M. Goldberg, D. Luce.Can exposure to very low levels of asbestos induce pleural mesothelioma ?.Am J Respir Crit Care Med, 172 (2005), pp. 939-940http://dx.doi.org/10.1164/rccm.2507003 | Medline[8]RT Lin, K. Takahashi, A. Karjalainen, T. Hoshuyama, D. Wilson, T. Kameda, et al .Ecological association between asbestos-related diseases and historical asbestos consumption: An international analysis.Lancet, 369 (2007), pp. 844-849http://dx.doi.org/10.1016/S0140-6736(07)60412-7 | Medline[9]C. Bianchi, T. Bianchi, S. Bucconi.Malignant mesothelioma of the pleura in nonagenarian patients.Tumori, 97 (2011), pp. 156-159http://dx.doi.org/10.1700/667.7776 | Medline[10]BW Robinson, RA Lake.Advances in malignant mesothelioma.N Engl J Med, 353 (2005), pp. 1591-1603http://dx.doi.org/10.1056/NEJMra050152 | Medline[eleven]ZJ Wang, GP Reddy, MB Gotway, CB Higgins, DM Jablons, M. Ramaswamy, et al .Malignant pleural mesothelioma: Evaluation with CT MR imaging, and PET.Radiographics, 24 (2004), pp. 105-119http://dx.doi.org/10.1148/rg.241035058 | Medline[12]S. Sharif, I. Zahid, T. Routledge, M. Scarci.Does positron emission tomography offer prognostic information in malignant pleural mesothelioma ?.Interact Cardiovasc Thorac Surg, 12 (2011), pp. 806-811http://dx.doi.org/10.1510/icvts.2010.255901 | Medline[13]S. Basu, B. Saboury, DA Torigian, A. Alavi.Current evidence base of FDG-PET / CT imaging in the clinical management of malignant pleural mesothelioma: Emerging significance of image segmentation and global disease assessment.Mol Imaging Biol, 13 (2011), pp. 801-811http://dx.doi.org/10.1007/s11307-010-0426-6 | Medline[14]I. Zahid, S. Sharif, T. Routledge, A. Alavi.What is the best way to diagnose and stage malignant pleural mesothelioma ?.Interact Cardiovasc Thorac Surg, 12 (2011), pp. 254-259http://dx.doi.org/10.1510/icvts.2010.255893 | Medline[fifteen]T. Shinohara, N. Shiota, M. Kume, N. Hamada, K. Naruse, F. Ogushi.Asymptomatic primary tuberculous pleurisy with intense 18-fluorodeoxyglucose uptake mimicking malignant mesothelioma.BMC Infect Dis, 13 (2013), pp. 12http://dx.doi.org/10.1186/1471-2334-13-12 | Medline[16]Y. Abe, K. Tamura, I. Sakata, J. Ishida, I. Fukuba, R. Matsuoka, et al .Usefulness of (18) F-FDG positron emission tomography / computed tomography for the diagnosis of pyothorax-associated lymphoma: A report of three cases.Oncol Lett, 1 (2010), pp. 833-836http://dx.doi.org/10.3892/ol_00000146 | Medline[17]T. Vandemoortele, S. Laroumagne, E. Roca, O. Bylicki, JP Dales, H. Dutau, et al .Positive FDG-PET / CT of the pleura twenty years after talc pleurodesis: Three cases of benign talcoma.Respiration, 87 (2014), pp. 243-248http://dx.doi.org/10.1159/000356752 | Medline[18]C. Plathow, A. Staab, A. Schmaehl, P. Aschoff, I. Zuna, C. Pfannenberg, et al .Computed tomography, positron emission tomography, positron emission tomography / computed tomography, and magnetic resonance imaging for staging of limited pleural mesothelioma: Initial results.Invest Radiol, 43 (2008), pp. 737-744http://dx.doi.org/10.1097/RLI.0b013e3181817b3d | Medline[19]N. Fujimoto, K. Gemba, M. Asano, Y. Fuchimoto, S. Wada, K. Ono, et al .Hyaluronic acid in the pleural fluid of patients with malignant pleural mesothelioma.Respir Investig, 51 (2013), pp. 92-97http://dx.doi.org/10.1016/j.resinv.2013.02.002 | Medline[twenty]J. Creaney, IM Dick, A. Segal, AW Musk, BW Robinson.Pleural effusion hyaluronic acid as a prognostic marker in pleural malignant mesothelioma.Lung Cancer, 82 (2013), pp. 491-498http://dx.doi.org/10.1016/j.lungcan.2013.09.016 | Medline[twenty-one]Y. Ogata, K. Aoe, A. Hiraki, K. Murakami, D. Kishino, K. Chikamori, et al .Is adenosine deaminase in pleural fluid a useful marker for differentiating tuberculosis from lung cancer or mesothelioma in Japan, a country with intermediate incidence of tuberculosis ?.Acta Med Okayama, 65 (2011), pp. 259-263Medline[22]F. Rodríguez-Panadero, MA Pérez, MA Moya, MI Cruz.Management of pleural pathology.Arch Bronconeumol, 45 (2009), pp. 22-27http://dx.doi.org/10.1016/S0300-2896(09)72854-6 | Medline[2. 3]DW Henderson, KB Shilkin, D. Whitaker.Reactive mesothelial hyperplasia vs mesothelioma, including mesothelioma in situ: A brief review.Am J Clin Pathol, 110 (1998), pp. 397-404Medline[24]DW Henderson, G. Reid, SC Kao, N. van Zandwijk, S. Klebe.Challenges and controversies in the diagnosis of mesothelioma: Part 1. Cytology-only diagnosis, biopsies, immunohistochemistry, discrimination between mesothelioma and reactive mesothelial hyperplasia, and biomarkers.J Clin Pathol, 66 (2013), pp. 847-853http://dx.doi.org/10.1136/jclinpath-2012-201303 | Medline[25]British Thoracic Society Standards of Care Committee BTS statement on malignant mesothelioma in the UK, 2007. Thorax. 2007; 62 Suppl 2: ii1-ii19.[26]AN Husain, T. Colby, N. Ordonez, T. Krausz, R. Attanoos, MB Beasley, et al .Guidelines for pathologic diagnosis of malignant mesothelioma: 2012 update of the consensus statement from the International Mesothelioma Interest Group.Arch Pathol Lab Med, 137 (2013), pp. 647-667http://dx.doi.org/10.5858/arpa.2012-0214-OA | Medline[27]N. Van Zandwijk, C. Clarke, D. Henderson, AW Musk, K. Fong, A. Nowak, et al .Guidelines for the diagnosis and treatment of malignant pleural mesothelioma.J Thorac Dis, 5 (2013), pp. E254-E307http://dx.doi.org/10.3978/j.issn.2072-1439.2013.11.28 | Medline[28]A. Scherpereel, P. Astoul, P. Baas, T. Berghmans, H. Clayson, P. de Vuyst, et al .Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma.Eur Respir J, 35 (2010), pp. 479-495http://dx.doi.org/10.1183/09031936.00063109 | Medline[29]NA Maskell, FV Gleeson, RJ Davies.Standard pleural biopsy versus CT-guided cutting-needle biopsy for diagnosis of malignant disease in pleural effusions: A randomized controlled trial.Lancet, 361 (2003), pp. 1326-1330Medline[30]M. Metintas, G. Ak, E. Dundar, H. Yildirim, R. Ozkan, E. Kurt, et al .Medical thoracoscopy vs CT scan-guided Abrams pleural needle biopsy for diagnosis of patients with pleural effusions: A randomized, controlled trial.Chest, 137 (2010), pp. 1362-1368http://dx.doi.org/10.1378/chest.09-0884 | Medline[31]JA Stigt, JE Boers, HJ Groen.Analysis of «dry» mesothelioma with ultrasound guided biopsies.Lung Cancer, 78 (2012), pp. 229-233http://dx.doi.org/10.1016/j.lungcan.2012.09.004 | Medline[32]RL Attanoos, AR Gibbs.The comparative accuracy of different pleural biopsy techniques in the diagnosis of malignant mesothelioma.Histopathology, 53 (2008), pp. 340-344http://dx.doi.org/10.1111/j.1365-2559.2008.03099.x | Medline[33]AR Medford, S. Agrawal, CM Free, JA Bennett.A local anesthetic video-assisted thoracoscopy service: Prospective performance analysis in a UK tertiary respiratory center.Lung Cancer, 66 (2009), pp. 355-358http://dx.doi.org/10.1016/j.lungcan.2009.02.023 | Medline[3. 4]F. Rodríguez-Panadero.Medical thoracoscopy.Respiration, 76 (2008), pp. 363-372http://dx.doi.org/10.1159/000158545 | Medline[35]J. Walters, NA Maskell.Biopsy techniques for the diagnosis of mesothelioma.Recent Results Cancer Res, 189 (2011), pp. 45-55http://dx.doi.org/10.1007/978-3-642-10862-4_4 | Medline[36]L. Greillier, A. Cavailles, A. Fraticelli, A. Scherpereel, F. Barlesi, G. Tassi, et al .Accuracy of pleural biopsy using thoracoscopy for the diagnosis of histologic subtype in patients with malignant pleural mesothelioma.Cancer, 110 (2007), pp. 2248-2252http://dx.doi.org/10.1002/cncr.23034 | Medline[37]SC Kao, TD Yan, K. Lee, J. Burn, DW Henderson, S. Klebe, et al .Accuracy of diagnostic biopsy for the histological subtype of malignant pleural mesothelioma.J Thorac Oncol, 6 (2011), pp. 602-605http://dx.doi.org/10.1097/JTO.0b013e31820ce2c7 | Medline[38]J. Creaney, RJ Francis, IM Dick, AW Musk, BW Robinson, MJ Byrne, et al .Identification of miRNA-103 in the cellular fraction of human peripheral blood as a potential biomarker for malignant mesothelioma – a serum soluble mesothelin concentrations in malignant pleural mesothelioma: Relationship to tumor volume, clinical stage and changes in tumor burden.Clin Cancer Res, 17 (2011), pp. 1181-1189http://dx.doi.org/10.1158/1078-0432.CCR-10-1929 | Medline[39]JA Rodríguez Portal.Asbestos-related disease: Screening and diagnosis.Adv Clin Chem, 57 (2012), pp. 163-185Medline[40]K. Hollevoet, JB Reitsma, J. Creaney, BD Grigoriu, BW Robinson, A. Scherpereel, et al .Serum mesothelin for diagnosing malignant pleural mesothelioma: An individual patient data meta-analysis.J Clin Oncol, 30 (2012), pp. 1541-1549http://dx.doi.org/10.1200/JCO.2011.39.6671 | Medline[41]CE Hooper, AJ Morley, P. Virgo, JE Harvey, B. Kahan, NA Maskell, et al .A prospective trial evaluating the role of mesothelin in undiagnosed pleural effusions.Eur Respir J, 41 (2013), pp. 18-24http://dx.doi.org/10.1183/09031936.00148211 | Medline[42]A. Cui, XG Jin, K. Zhai, ZH Tong, HZ Shi.Diagnostic values of soluble mesothelin-related peptides for malignant pleural mesothelioma: updated meta-analysis.BMJ Open, 4 (2014), pp. e004145http://dx.doi.org/10.1136/bmjopen-2013-004145 | Medline[43]I. Pantazopoulos, P. Boura, T. Xanthos, K. Syrigos.Effectiveness of mesothelin family proteins and osteopontin for malignant mesothelioma.Eur Respir J, 41 (2013), pp. 706-715http://dx.doi.org/10.1183/09031936.00226111 | Medline[44]HI Pass, SM Levin, MR Harbut, J. Melamed, L. Chiriboga, J. Donington, et al .Fibulin-3 as a blood and effusion biomarker for pleural mesothelioma.N Engl J Med, 367 (2012), pp. 1417-1427http://dx.doi.org/10.1056/NEJMoa1115050 | Medline[Four. Five]HI Pass, D. Lott, F. Lonardo, M. Harbut, Z. Liu, N. Tang, et al .Asbestos exposure, pleural mesothelioma, and serum osteopontin levels.N Engl J Med, 353 (2005), pp. 1564-1573http://dx.doi.org/10.1056/NEJMoa051185 | Medline[46]F. Gueugnon, S. Leclercq, C. Blanquart, C. Sagan, L. Cellerin, M. Padieu, et al .Identification of novel markers for the diagnosis of malignant pleural mesothelioma.Am J Pathol, 178 (2011), pp. 1033-1042http://dx.doi.org/10.1016/j.ajpath.2010.12.014 | Medline[47]DW Henderson, G. Reid, SC Kao, N. van Zandwijk, S. Klebe.Challenges and controversies in the diagnosis of malignant mesothelioma: Part 2. Malignant mesothelioma subtypes, pleural synovial sarcoma, molecular and prognostic aspects of mesothelioma, BAP1, aquaporin-1 and microRNA.J Clin Pathol, 66 (2013), pp. 854-861http://dx.doi.org/10.1136/jclinpath-2013-201609 | Medline[48]I. Bentwich, A. Avniel, Y. Karov, R. Aharonov, S. Gilad, O. Barad, et al .Identification of hundreds of conserved and nonconserved human microRNAs.Nat Genet, 37 (2005), pp. 766-770http://dx.doi.org/10.1038/ng1590 | Medline[49]H. Benjamin, D. Lebanony, S. Rosenwald, L. Cohen, H. Gibori, N. Barabash, et al .A diagnostic assay based on microRNA expression accurately identifies malignant pleural mesothelioma.J Mol Diagn, 12 (2010), pp. 771-779http://dx.doi.org/10.2353/jmoldx.2010.090169 | Medline[fifty]DG Weber, G. Johnen, O. Bryk, KH Jöckel, T. Brüning.Identification of miRNA-103 in the cellular fraction of human peripheral blood as a potential biomarker for malignant mesothelioma. A pilot study.PLoS One, 7 (2012), pp. e30221http://dx.doi.org/10.1371/journal.pone.0030221 | Medline[51]VW Rusch, D. Giroux, C. Kennedy, E. Ruffini, AK Cangir, D. Rice, et al .Initial analysis of the international association for the study of lung cancer mesothelioma database.J Thorac Oncol, 7 (2012), pp. 1631http://dx.doi.org/10.1097/JTO.0b013e31826915f1 | Medline[52]JP Van Meerbeeck, A. Scherpereel, VF Surmont, P. Baas.Malignant pleural mesothelioma: The standard of care and challenges for future management.Crit Rev Oncol Hematol, 78 (2011), pp. 92-111http://dx.doi.org/10.1016/j.critrevonc.2010.04.004 | Medline[53]PM McCormack, F. Nagasaki, BS Hilaris, N. Martini.Surgical treatment of pleural mesothelioma.J Thorac Cardiovasc Surg, 84 (1982), pp. 834-842Medline[54]RM Flores.Surgical options in malignant pleural mesothelioma: Extrapleural pneumonectomy or pleurectomy / decortication.Semin Thorac Cardiovasc Surg, 21 (2009), pp. 149-153http://dx.doi.org/10.1053/j.semtcvs.2009.06.008 | Medline[55]AS Wolf, J. Daniel, DJ Sugarbaker.Surgical techniques for multimodality treatment of malignant pleural mesothelioma: Extrapleural pneumonectomy and pleurectomy / decortication.Semin Thorac Cardiovasc Surg, 21 (2009), pp. 132-148http://dx.doi.org/10.1053/j.semtcvs.2009.07.007 | Medline[56]O. Rena, C. Casadio.Extrapleural pneumonectomy for early stage malignant pleural mesothelioma: A harmful procedure.Lung Cancer, 77 (2012), pp. 151-155http://dx.doi.org/10.1016/j.lungcan.2011.12.009 | Medline[57]DJ Sugarbaker, JP Garcia.Multimodality therapy for malignant pleural mesothelioma.Chest, 112 (1997), pp. 272S-275SMedline[58]WG Richards, L. Zellos, R. Bueno, MT Jaklitsch, PA Jänne, LR Chirieac, et al .Phase I to ii study of pleurectomy / decortication and intraoperative intracavitary hyperthermic cisplatin lavage for mesothelioma.J Clin Oncol, 24 (2006), pp. 1561-1567http://dx.doi.org/10.1200/JCO.2005.04.6813 | Medline[59]PE Van Schil, P. Baas, R. Gaafar, AP Maat, M. Van de Pol, B. Hasan, et al .Diagnostic values of soluble mesothelin-related peptides for malignant pleural mesothelioma: Updated meta-analysis.BMJ Open, 36 (2010), pp. 1362-1369[60]RM Flores, HI Pass, VE Seshan, J. Dycoco, M. Zakowski, M. Carbone, et al .Extrapleural pneumonectomy versus pleurectomy / decortication in the surgical management of malignant pleural mesothelioma: Results in 663 patients.J Thorac Cardiovasc Surg, 135 (2008), pp. 620-626http://dx.doi.org/10.1016/j.jtcvs.2007.10.054 | Medline[61]JC Halstead, E. Lim, RM Venkateswaran, SC Charman, M. Goddard, AJ Ritchie.Improved survival with VATS pleurectomy-decortication in advanced malignant mesothelioma.Eur J Surg Oncol, 31 (2005), pp. 314-320http://dx.doi.org/10.1016/j.ejso.2004.08.014 | Medline[62]MJ Weyant.Is it time to consider pleurectomy and decortication as the only surgical treatment for malignant pleural mesothelioma ?.J Thorac Oncol, 7 (2012), pp. 629-630http://dx.doi.org/10.1097/JTO.0b013e31824d9a52 | Medline[63]AE Martin-Ucar, A. Nakas, JG Edwards, DA Waller.Case-control study between extrapleural pneumonectomy and radical pleurectomy / decortication for pathological N2 malignant pleural mesothelioma.Eur J Cardiothorac Surg, 31 (2007), pp. 765-770http://dx.doi.org/10.1016/j.ejcts.2007.01.064 | Medline[64]T. Treasure, L. Lang-Lazdunski, D. Waller, JM Bliss, C. Tan, J. Entwisle, et al .Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: Clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomized feasibility study.Lancet Oncol, 12 (2011), pp. 763-772http://dx.doi.org/10.1016/S1470-2045(11)70149-8 | Medline[65]W. Weder, RA Stahel, P. Baas, U. Dafni, M. de Perrot, BC McCaughan, et al .The MARS feasibility trial: Conclusions not supported by data.Lancet Oncol, 12 (2011), pp. 4-5http://dx.doi.org/10.1016/S1470-2045(10)70280-1 | Medline[66]L. Lang-Lazdunski, A. Bille, R. Lal, P. Cane, E. McLean, D. Landau, et al .Pleurectomy / decortication is superior to extrapleural pneumonectomy in the multimodality management of patients with malignant pleural mesothelioma.J Thorac Oncol, 7 (2012), pp. 737-743http://dx.doi.org/10.1097/JTO.0b013e31824ab6c5 | Medline[67]E. Minatel, M. Trovo, J. Polesel, IA Rumeileh, T. Baresic, A. Bearz, et al .Tomotherapy after pleurectomy / decortication or biopsy for malignant pleural mesothelioma allows the delivery of high dose of radiation in patients with intact lung.J Thorac Oncol, 7 (2012), pp. 1862-1866http://dx.doi.org/10.1097/JTO.0b013e318272601f | Medline[68]A. Price.What is the role of radiotherapy in malignant pleural mesothelioma ?.Oncologist, 16 (2011), pp. 359-365http://dx.doi.org/10.1634/theoncologist.2010-0185 | Medline[69]L. De Graaf-Strukowska, J. Van der Zee, W. Van Putten, S. Senan.Factors influencing the outcome of radiotherapy in malignant mesothelioma of the pleura – a single-institution experience with 189 patients.Int J Radiat Oncol Biol Phys, 43 (1999), pp. 511-516Medline[70]P. Jenkins, R. Milliner, C. Salmon.Re-evaluating the role of palliative radiotherapy in malignant pleural mesothelioma.Eur J Cancer, 47 (2011), pp. 2143-2149http://dx.doi.org/10.1016/j.ejca.2011.05.012 | Medline[71]EM Low, GG Khoury, AW Matthews, E. Neville.Prevention of tumor seeding following thoracoscopy in mesothelioma by prophylactic radiotherapy.Clin Oncol (R Coll Radiol), 7 (1995), pp. 317-318[72]D. De Ruysscher, B. Slotman.Treatment of intervention sites of malignant pleural mesothelioma with radiotherapy: A Dutch-Belgian survey.Radiother Oncol, 68 (2003), pp. 299-302Medline[73]DA Fennell, G. Gaudino, KJ O’Byrne, L. Mutti, J. Van Meerbeeck.Advances in the systemic therapy of malignant pleural mesothelioma.Nat Clin Pract Oncol, 5 (2008), pp. 136-147http://dx.doi.org/10.1038/ncponc1039 | Medline[74]AK Nowak.Chemotherapy for malignant pleural mesothelioma: A review of current management and a look to the future.Ann Cardiothorac Surg, 1 (2012), pp. 508-515http://dx.doi.org/10.3978/j.issn.2225-319X.2012.10.05 | Medline[75]JN Jakobsen, JB Sorensen.Review on clinical trials of targeted treatments in malignant mesothelioma.Cancer Chemother Pharmacol, 68 (2011), pp. 1-15http://dx.doi.org/10.1007/s00280-011-1655-3 | Medline[76]R. Hassan, E. Sharon, I. Pastan.Mesothelin targeted chemo-immunotherapy for treatment of malignant mesothelioma and lung adenocarcinoma.Ann Oncol, (2010),[77]RM Wong, I. Ianculescu, S. Sharma, DL Gage, OM Olevsky, S. Kotova, et al .Immunotherapy for malignant pleural mesothelioma. Current status and future prospects.Am J Respir Cell Mol Biol, 50 (2014), pp. 870-875http://dx.doi.org/10.1165/rcmb.2013-0472TR | Medline[78]JP Hegmans, JD Veltman, ME Lambers, IJ de Vries, CG Figdor, RW Hendriks, et al .Consolidative dendritic cell-based immunotherapy elicits cytotoxicity against malignant mesothelioma.Am J Respir Crit Care Med, 181 (2010), pp. 1383-1390http://dx.doi.org/10.1164/rccm.200909-1465OC | Medline[79]P. Astoul, E. Roca, F. Gallateau-Salle, A. Scherpereel.Malignant pleural mesothelioma. From the bench to the bedside.Respiration, 83 (2012), pp. 481-493http://dx.doi.org/10.1159/000339259 | Medline[80]H. Kim, W. Gao, M. Ho.Novel immunocytokine IL12-SS1 (Fv) inhibits mesothelioma tumor growth in nude mice.PLoS One, 8 (2013), pp. e81919http://dx.doi.org/10.1371/journal.pone.0081919 | Medline[81]F. Rodriguez-Panadero, A. Montes-Worboys.Mechanisms of pleurodesis.Respiration, 83 (2012), pp. 91-98http://dx.doi.org/10.1159/000335419 | Medline[82]S. Bielsa, P. Hernández, F. Rodriguez-Panadero, T. Taberner, A. Salud, JM Porcel.Tumor type influences the effectiveness of pleurodesis in malignant effusions.Lung, 189 (2011), pp. 151-155http://dx.doi.org/10.1007/s00408-011-9283-6 | Medline[83]E. Cases, L. Seijo, C. Disdier, MJ Lorenzo, R. Cordovilla, F. Sanchis, et al .Use of permanent pleural drainage in outpatient management of recurrent malignant pleural effusion.Arch Bronconeumol, 45 (2009), pp. 591-596http://dx.doi.org/10.1016/j.arbres.2009.09.009 | Medline[84]ME Van Meter, KY McKee, RJ Kohlwes.Efficacy and safety of tunneled pleural catheters in adults with malignant pleural effusions: A systematic review.J Gen Intern Med, 26 (2011), pp. 70-76http://dx.doi.org/10.1007/s11606-010-1472-0 | Medline[85]HE Davies, EK Mishra, BC Kahan, JM Wrightson, AE Stanton, A. Guhan, et al .Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion. The TIME2 randomized controlled trial.JAMA, 307 (2012), pp. 2383-2389http://dx.doi.org/10.1001/jama.2012.5535 | Medline[86]MJ Lorenzo, M. Modesto, J. Pérez, E. Bollo, R. Cordovilla, M. Muñoz, et al .Quality-of-life assessment in malignant pleural effusion treated with indwelling pleural catheter: A prospective study.Palliat Med, 28 (2014), pp. 326-334http://dx.doi.org/10.1177/0269216314521851 | Medline[87]C. Alberti.From molecular imaging in preclinical / clinical oncology to theranostic applications in targeted tumor therapy.Eur Rev Med Pharmacol Sci, 16 (2012), pp. 1925-1933Medline[88]H. Zhang, M. Tian, E. Li, Y. Fujibayashi, LH Shen, DJ Yang.Molecular imaging-guided theranostics and personalized medicine.J Biomed Biotechnol, 2012 (2012), pp. 747416http://dx.doi.org/10.1155/2012/747416 | Medline[89]S. Bidlingmaier, J. He, Y. Wang, F. An, J. Feng, D. Barbone, et al .Identification of MCAM / CD146 as the target antigen of a human monoclonal antibody that recognizes both epithelioid and sarcomatoid types of mesothelioma.Cancer Res, 69 (2009), pp. 1570-1577http://dx.doi.org/10.1158/0008-5472.CAN-08-1363 | Medline[90]Y. Hama, Y. Urano, Y. Koyama, M. Kamiya, M. Bernardo, RS Paik, et al .A target cell-specific activatable fluorescence probe for in vivo molecular imaging of cancer based on a self-quenched Avidin-Rhodamine conjugate.Cancer Res, 67 (2007), pp. 2791-2799http://dx.doi.org/10.1158/0008-5472.CAN-06-3315 | Medline[91]V. Ntziachristos, C. Bremer, R. Weissleder.Fluorescence imaging with near-infrared light: New technological advances that enable in vivo molecular imaging.Eur Radiol, 13 (2003), pp. 195-208http://dx.doi.org/10.1007/s00330-002-1524-x | Medline[92]AM Morawski, PM Winter, KC Crowder, SD Caruthers, RW Fuhrhop, MJ Scott, et al .Targeted nanoparticles for quantitative imaging of sparse molecular epitopes with MRI.Magn Reson Med, 51 (2004), pp. 480-486http://dx.doi.org/10.1002/mrm.20010 | Medline[93]TK Nayak, M. Bernardo, DE Milenic, PL Choyke, MW Brechbiel.Orthotopic pleural mesothelioma in mice: SPECT / CT and MR imaging with HER1- and HER2-targeted radiolabeled antibodies.Radiology, 26 (2013), pp. 173-182[94]RM Ostroff, MR Mehan, A. Stewart, D. Ayers, EN Brody, SA Williams, et al .Early detection of malignant pleural mesothelioma in asbestos-exposed individuals with a noninvasive proteomics-based surveillance tool.PLoS One, 7 (2012), pp. e46091http://dx.doi.org/10.1371/journal.pone.0046091 | Medline[95]F. Mundt, HJ Johansson, J. Forshed, S. Arslan, M. Metintas, K. Dobra, et al .Proteome screening of pleural effusions identifies galectin 1 as a diagnostic biomarker and highlights several prognostic biomarkers for malignant mesothelioma.Mol Cell Proteomics, 13 (2014), pp. 701-715http://dx.doi.org/10.1074/mcp.M113.030775 | Medline[96]A. Vachani, E. Moon, SM Albelda.Gene therapy for mesothelioma.Curr Treat Options Oncol, 12 (2011), pp. 173-180http://dx.doi.org/10.1007/s11864-011-0153-5 | Medline[97]AR Haas, DH Sterman.Novel intrapleural therapies for malignant diseases.Respiration, 83 (2012), pp. 277-292http://dx.doi.org/10.1159/000337060 | Medline[98]Y. Tada, H. Shimada, K. Hiroshima, M. Tagawa.A potential therapeutic strategy for malignant mesothelioma with gene medicine.Biomed Res Int, 2013 (2013), pp. 572609http://dx.doi.org/10.1155/2013/572609 | Medline[99]O. Melaiu, J. Stebbing, Y. Lombardo, E. Bracci, N. Uehara, A. Bonotti, et al .MSLN gene silencing has an anti-malignant effect on cell lines overexpressing mesothelin deriving from malignant pleural mesothelioma.PLoS One, 9 (2014), pp. e85935http://dx.doi.org/10.1371/journal.pone.0085935 | Medline





[…] Diagnosis and treatment of malignant pleural mesothelioma markers […]
[…] Diagnosis and treatment of malignant pleural mesothelioma markers […]